

Batch data from COVID-19 vaccines in Australia suggests massive underreporting in most batches
It looks like the medical professionals report their own AEs more than AEs are reported for the general public

I have been trying to get batch (or lot) data on records associated with suspected Adverse Events (AEs) from the COVID-19 vaccines from the Therapeutic Goods Administration (TGA) since December 2021. The reason for wanting this information was the enormously different levels of AEs, disabilities and deaths in some batches reported on VAERS (Vaccine Adverse Event Reporting System) based in the USA. I wanted to see if the same pattern from VAERS emerged from the Australian data set. Finally on 25 March 2022 I received something useful with the release of TGA FOI-3545 (there is a story here which I will go into in my next post).
I had a failed FOI request with the Department of Health (FOI 3467) which would have provided the number of doses administered per batch. Interestingly, the Department prepared the information in a document 'COVID-19 Vaccine Batch Data Extract 12/01/2022' but then consulted with 3rd parties and decided to prevent release. Some of the reasons for preventing the release included trade secrets, commercially valuable information and undermining industry confidence in confidentiality (more info here). It is just the number of doses administered per batch, but somehow that needs to be kept secret from the public that paid for all of this. I am still attempting to get a small normalised subset of that information via a new FOI request. Until just recently I thought it would be possible, but the request is now in the hands of the 3rd parties involved and apparently up to them (it's probably not going to happen).
{kind=link}
{kind=link}
At the time that I submitted the request for FOI-3545 I also requested any documents that compared the AEs and deaths from different batches of COVID-19 vaccines (FOI-3546). The response was:
{kind=link}
Unfortunately, I am unable to continue to process your request because the documents you have requested do not exist.
This surprised me. The response mentioned that they aim to detect patterns of events that indicate a 'safety signal', but I was naively expecting that the TGA would generate regular detailed internal reports to closely monitor these new experimental vaccines. I thought the unusual situation of a rushed vaccine would warrant an extreme level of attention from the TGA.
Important Medical Events
The European Medicines Agency (EMA) publishes a list of Important Medical Events (IMEs). This list of reaction terms was used to sort out the less important AEs from the more important ones (headaches and sore arms are not that important, and there is probably a greater variance in reporting of less important events). Figure 1 shows the number of cases with IMEs per batch for Pfizer vaccine batches by the initial release date. Unfortunately, this graph isn't particularly useful without the number of doses administered per batch (which for some reason we will probably never be allowed to know).

Figure 1. Number of cases containing Important Medical Events from suspected Adverse Events from a Pfizer COVID-19 vaccine by initial release date.
Figure 2 plots the suspected IMEs from the Pfizer batches against all AEs from the same batch. This may indicate that some batches received better reporting than other batches. Figure 3 shows the same information as Figure 2, with grouping of the first three, the next eight and all other batches with associated trend lines. In the first three batches, about 12% of reports contained IMEs. About 15% of reports contained IMEs in the next eight batches. For all other batches, about 25% of reports contained IMEs.
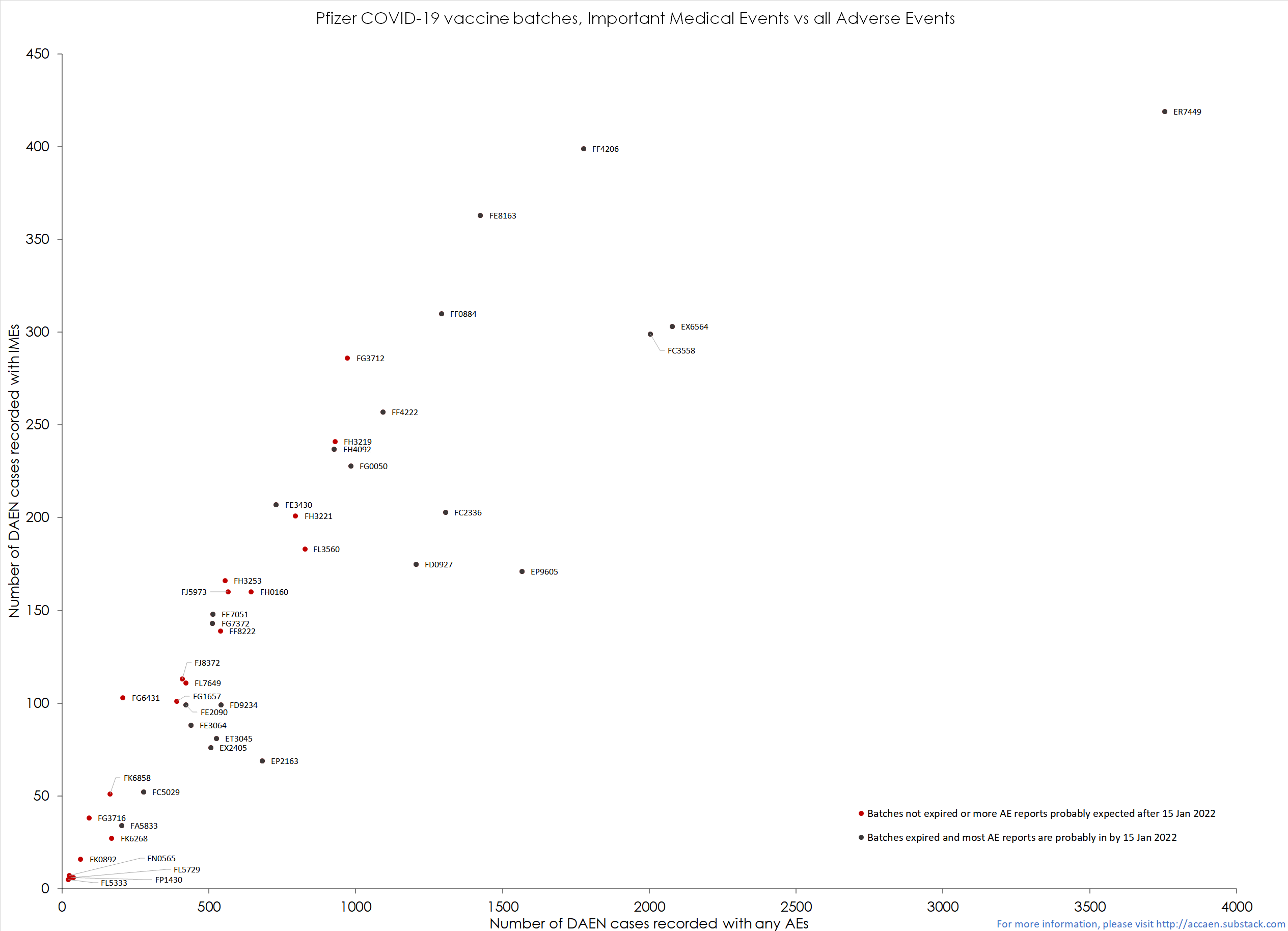
Figure 2. Plot of Important Medical Events vs all suspected Adverse Events from Pfizer COVID-19 vaccine batches.

Figure 3. Plot of Important Medical Events vs all suspected Adverse Events from Pfizer COVID-19 vaccine batches grouped by release periods.
The first doses of vaccines (phase 1a) were given to frontline healthcare workers, aged care and disability care residents and workers, and quarantine and border workers. The following group of recipients (phase 1b) included all other healthcare workers, adults 70 years and older, aboriginal adults 55 years and older, adults with underlying medical conditions, and emergency service workers. A feasible explanation for the differing ratios of IMEs to AEs is that healthcare professionals understand the reporting system better and are more likely to report any adverse event. Healthcare workers probably represented a higher proportion of doses administered in phase 1a than phase 1b. Phase 1b would have had a higher proportion of healthcare workers than later phases. This probably also means that underreporting in later batches is worse, but that is not clear without the number of doses administered per batch.
It is possible that some batches could be more dangerous than others, however, the available data sets from the TGA don't provide enough information to adequately test this hypothesis. We can observe differences in the ratio of all AEs vs IMEs across batches, which seems to indicate better levels of reporting of AEs from batches administered to higher proportions of medical professionals. This seems to align with the conclusions of Leonard Frey discussed here and here.
I welcome anyone to take the data sets presented in FOI-3545 (also here) and DAEN and let me know if the findings are the same or different.
I hadn't heard of Leonard Frey's idea before. This might be hinted at by VAERS narrative fields. I'll run a RegEx on it.